
|
Quad ACL ReconstructionSurgery is typically recommended to help patients get back to their level of pre-injury activity. Dr. Saper performs ACL reconstruction surgery using an arthroscopic approach to reconstruct the damaged ACL. During arthroscopic knee surgery, Dr. Saper uses small incisions on the knee to insert a camera, as well as surgical tools to evaluate the ligament and other structures inside the knee.
In most cases, Dr. Saper will need to use a graft to reconstruct the ligament. Grafts can be harvested from the patient (autograft) or can be acquired from a donor (allograft). Each case is unique, and decisions are individualized, based upon a given patient’s age, activity level, goals, and history. Dr. Saper will review all options prior to surgery. Following ACL reconstruction surgery, Dr. Saper will construct a thorough rehabilitation program that should be fulfilled in its entirety. After surgery patients are fitted with a brace and use crutches until their quadriceps muscle returns in strength. Therapy and the use of functional braces will be individualized to the exact injury and patient’s needs. To learn more about ACL injuries, or for additional information on ACL reconstruction, please contact the Seattle, WA orthopedic surgeon, Dr. Michael Saper located at Seattle Children's. |
|
|
Meniscus SurgeryFor larger tears, those that have failed non-operative management, and those with frank mechanical symptoms, surgery is typically recommended.
A meniscectomy will be performed on the knee if the meniscus has a small symptomatic tear, one that is shredded beyond repair, or a tear in the inner third of the meniscus. This procedure essentially removes the area of the tear, and removes the damaged section. This is called a partial meniscectomy. Dr. Saper will take great care to only remove the damaged part of the tear and leave as much of the healthy meniscus as possible. For tears that occur in the outer two thirds of the meniscus, or for larger tears that can be fixed, an attempt is made to repair the meniscus and preserve as much of the native meniscus as possible. This is performed with a combination arthroscopic and open procedure. Strong stitches are placed through the tear to bring the tissue back together and complete the repair. For a partial meniscectomy procedure, the patient is allowed to weight-bear as tolerated. After a meniscal repair, the knee must be protected to allow the meniscus to heal. Physical therapy is started immediately to regain motion and strength. Weight bearing is protected on crutches for two weeks followed by full weight bearing in the brace, which is worn for a total of six weeks. To learn more about mensical injuries of the knee, or for additional information on meniscus repairs or meniscus surgery of the knee, please contact the Seattle, WA orthopedic surgeon, Dr. Michael Saper located at Seattle Children's. |
|
|
IT Band Tenodesis or ALL / Extra-articular ReconstructionACL graft failure is a significant issue, particular in young athletes participating in high-demand pivoting and contact sports. In select patients after an ACL injury, or in the setting of a revision ACL reconstruction, Dr. Saper may recommend an anterolateral ligament (ALL) or lateral extra-articular reconstruction (IT Band tenodesis). The intent of the procedure is to better restore knee stability and further injury to the already compromised joint.
In some cases, Dr. Saper will use a strip of the patient's iliotibial band to reconstruct the ligament. In others, the graft can be acquired from a donor (allograft). Each case is unique, and decisions are individualized, based upon a given patient’s age, activity level, goals, and history. Dr. Saper will review all options prior to surgery. To learn more about ACL injuries, or for additional information on lateral extra-articular reconstruction procedures of the knee, please contact the Seattle, WA orthopedic surgeon, Dr. Michael Saper located at Seattle Children's. |
|
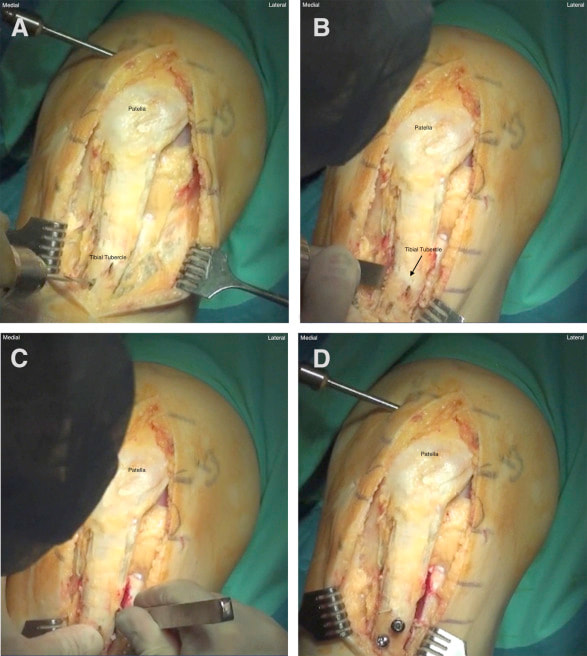
Patella RealignmentFor patients with patella instability that have failed non-operative management surgery is typically recommended. In patients with lateral patella subluxation/dislocation, Dr. Saper will typically recommend an MPFL reconstruction to stabilize the patella. In many cases, Dr. Saper will recommend a tibial tubercle osteotomy.
The tibial tubercle is undercut and freed from the tibia. The tubercle is pivoted slightly from lateral to medial to match the alignment of the patellar tendon. The angulation between the patellar tendon and tibial tubercle is corrected. The tibial tubercle is fixed with two screws. This change straightens the patellar tendon mechanism, reduces the lateral pull on the patella, and decreases pressure on the patella. The gap created by the lateral release is closed with a flap of the iliotibial band rotated upward to stabilize the lateral side of the patella. After surgery patients are fitted with a brace and use crutches until their quadriceps muscle returns in strength. Therapy and the use of functional braces will be individualized to the exact injury and patient’s needs. To learn more about patellofemoral conditions, or for additional information on patellofemoral surgery of the knee, please contact the Seattle, WA orthopedic surgeon, Dr. Michael Saper located at Seattle Children's. |